Assalamualaikum w.b.t
Today, I would like to share my knowledge about Tropia Classification. I start with ESOTROPIA.
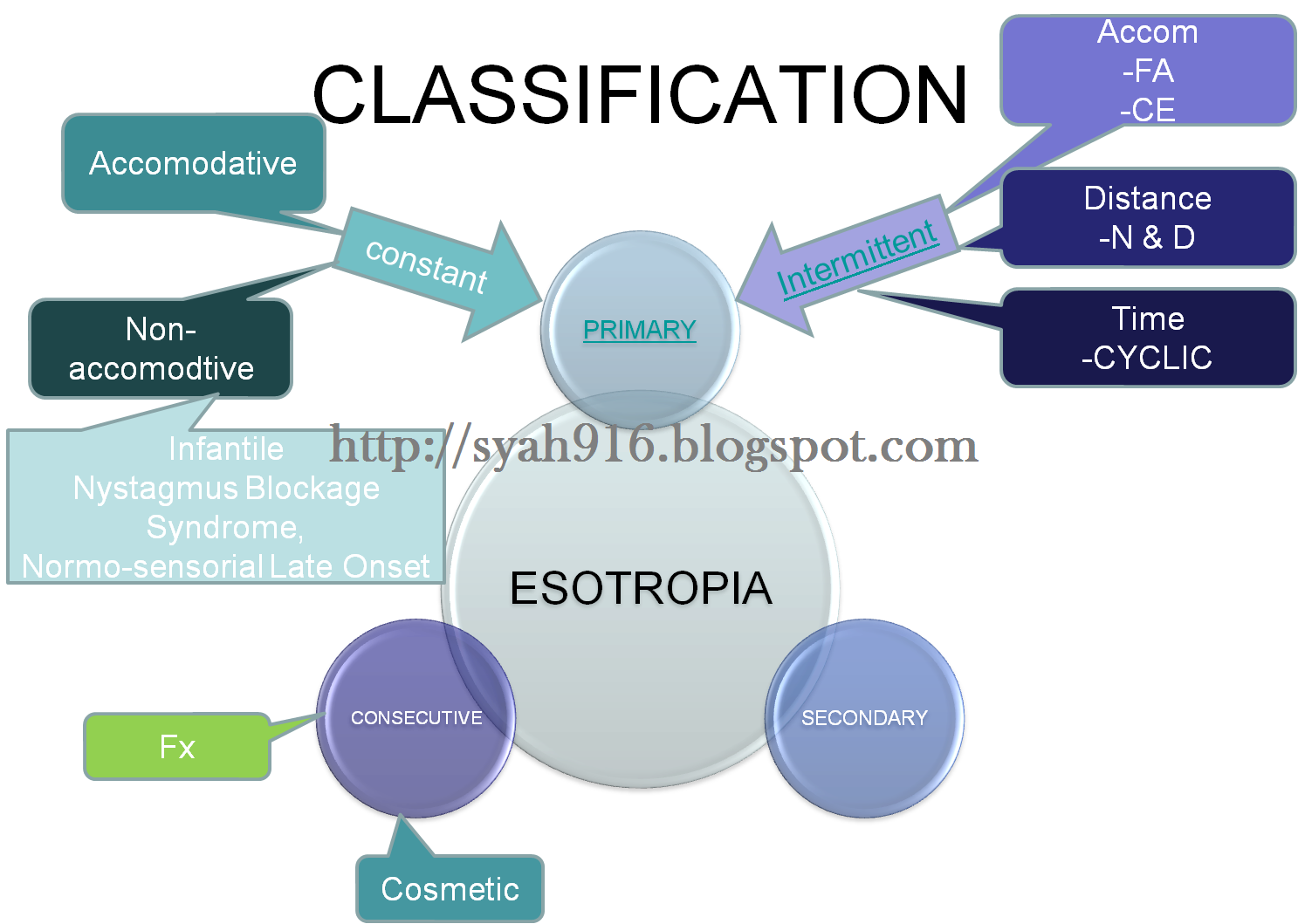
Basicly, esotropia can be classified into three type which are;
- Primary
- Secondary
- Consecutive
For Primary Esotopia will be divided into 2 types which are Constant and Intermittent type. For Constant, will be categorized to Accommodative and Non-accomodative and for Intermittent will be categorized to Accommodative, Distance and Time.
Secondary Esotropia could be caused by visual impairment, ocular trauma, certain ocular disease and etc.
Consecutive Esotropia could be caused by squint surgery procedure and can be classified as a functional and cosmetic case.
To ease your understanding, please refer to this figure.
In next post, I will explain further for each type of ESOTROPIA.

what a nice post we have here. I good to have it from expert. 'Tiada was-was pada faktanya'...yes
ReplyDeleteToday, I got an interesting case. Consecutive exotropia due to overcorrecting esotopia during surgery. 6pd XT was induced. He is anisometropia as well..
Frens, you can hv a look at his file later.
salam sir,
ReplyDeletecould you please explain further about the intermittent esotropia for distance and time?
@eli aimi
ReplyDeleteW'slm
I will explain further in our lecture today..
what are diff btwn esotropia ....:p
ReplyDelete@MD MUZIMAN SYAH
ReplyDeleteape ni..soalan tak lengkap
Farah Nadianah Question
ReplyDelete2. Why do you need differentiate constant accommodative esotropia and intermittent accommodative esotropia?
Izul Question,
ReplyDeletePlease write Esotropia classification in general and brief using layman language and term.
one in Malay version and in English version.
Nur Izzah Question
ReplyDeletePlease write Accommodative Constant Esotropia iin details using layman language and term.
one in Malay version and in English version.
please insert at least 2 diagram for your writing
For izul;
ReplyDeleteplease insert at least 3 diagram to explain your writing..you are allowed to use my diagram for eso classifaction
shahril's question
ReplyDeletePlease write Non Accommodative Constant Esotropia iin details using layman language and term.
one in Malay version and in English version.
please insert at least 2 diagram for your writingS
Correction for Izzah & Shahril questions
ReplyDeleteIzah, please write accommodative and non-accommodative constant esotropia
shahril, intermttent accommodatvie esotropia.
Zanariah's question
ReplyDeletePlease write Distance (near and Distance) & Time intermittent Esotropia iin details using layman language and term.
one in Malay version and in English version.
please insert at least 2 diagram for your writing
To Izul, Zana, Sharil, Izah only
ReplyDeleteall of your assignment must submit to me via both of these email; ioptoss@yahoo.com and dtravelog@yahoo.com before 12pm this Sunday
To all 3 rd year,
ReplyDeleteplease follow this blog using Google friend connect and networked blog & Like box using your FB account
please do it before submit your tutorial
Why do you need differentiate infantile esotropia and pseudoesotropia?
ReplyDeleteInfantile esotropia or congenital esotropia is a type of strabismus which is first appears sometimes within the first six month of life. These type of children often alternate their vision between two eyes. But some children constantly cross the same eyes,\. This indicated strabismus or decreased vision in one eye.
For psudoesotropia, is a condition in which the alignment of the eyes is straight. However they appear to be crossed. common in infants and younger children who have a broad, flat bridge of the nose which allows the skin on the inner part of the eyelids to extend over and cover the inner part of the eye(epicanthus fold).
We need to differentiate it because we do not want to give wrong treatment. If the baby only get pseudoesotropia but because of wrong diagnosis, we give the baby strabismic treatment such as patching. The result will be the worse. If we can differentiate the esotropia, we can plan how to manage the patient well. Wallahu ‘alam
:X
question 12: What are importance of measuring AC/A in tropia management?
ReplyDelete- the AC/A ratio can be usefully employed to assess the effect of the refractive correction on the ocular motor balance whilst considering management options in binocular vision management.
-assessment of the ratio between accommodation
and accommodative convergence(AC/A) ratio is important in treating patients with strabismus. this is because the influence it has on the type of tropia and also choice of treatment.
- bifocals are often prescribed for esotropes with a high AC/A ratio, in order to eliminate or decrease the angle at near to a size controllable by the compensating divergence.
-a high AC/A ratio means that accommodation causes a large change in convergence.in most divergence excess exotropia exhibits a high AC/A ratio, so that a minus overcorrection lens may be very effective in decreasing the size of the far point exodeviations and in stimulating the needed fusional convergence.
-the size at all distances or the AC/A must be considered when predicting the need for or the success of surgery.
Q11: for infantile esotropia case, when is the best time should be referred for surgery.
ReplyDeleteA:The exact timing for infantile esotropia surgery is still undetermined. In the North America, the typical age of surgery ranges from 11-18months. However in many parts of Western Europe, surgery is delayed until 2-4 years of age. Despite successful surgical realignment of the eyes, subnormal stereopsis and ocular motor deficit often persists. Recently, surgery at or before age 11months has been shown that it can restores binocular vision ,stereopsis and static eye alignment.
Furthermore, if the surgery are performed before 12month, the rate of success is around 71%, and if the surgery is performed at the age of 13-24 months, the rate of success is around 43%, and if the surgery is performed after age of 24months, the rate of success is only 12%.
As an optometrist, we must follow the patient with infantile esotropia for about two or three consecutive visits to check the stability of the strabismic deviation and allow the practitioner to elicit the possible existence of overreacting inferior oblique muscle, a dissociation vertical deviation or a nonconcomitant nature of the deviation before surgery.
Q1: What are the differences between constant accommodative esotropia and intermittent accommodative esotropia?
ReplyDeleteConstant accommodative esotropia:
1)Onset usually at 3-4 years of age.
2)Associated with hyperopia, astigmatism and anisometropia.
3)Constant deviation are normally unilateral and result in the typical secondary defect associated with such condition eg: amblyopia.
4)Also known as partial accommodative esotropia
5)A partially accommodative esotropia is present without spectacles and is reduced but not eliminated by the wearing of hyperopia prescription.
6)Management: correction of refractive error and treatment of amblopia. Surgery may be required for a cosmetic or functional result in cases that are not fully accommodative. Some cases can be straightened at near with bifocals.
Intermittentent accommodative esotropia:
1)Usually occurs at 2-5 years of age
2)Associated with a moderate degree of hyperopia.
3)The deviation is present only under certain condition and is unlikely to cause amblopia.
4)Consist of fully accommodative esotropia and convergence excess.
5)Binocular single vision is present for all distance when the hyperopia is corrected. Prescribe the appropriate amount of hyperopia needed to eliminate the strabismus.
6)Management: Full cycloplegic refraction correction is important, to prevent the occurrence of a partially accommodative esotropia and associated amblyopia. Orthoptic exercise can be used with older children to control manifest deviation.
Q8 : WHY WE NEED TO DIFFERENTIATE BETWEEN CONVERGENCE EXCESS AND NEAR ESOTROPIA?
ReplyDeleteWe need to differentiate between convergence excess and near esotropia because these 2 types have difference management.
Management for convergence excess is using base out prism in early management consideration. Because of the effectiveness of added lenses, prism is rarely necessary for convergence excess associated with normal tonic vergence (orthophoria at distance). In many cases of convergence excess, the use of added lens and prism will be sufficient to successfully treat the patient compared to vision therapy in divergence excess.
Near esotropia is a type of nonaccomodative convergence excess. In management for near esotropia, bifocal spectacles, miotic drugs and orthoptics treatment have no effect on this type of esotropia. However patient should be refracted and any significant refractive error corrected. Prism may be used to maintain BSV for near as temporary measure.
Question 10 :Why do you need to differentiate distance esotropia from mild 6th nerve palsy?
ReplyDeleteFrom my point of view,
We need to differentiate distance esotropia from mild 6th nerve palsy in order to
- Have a correct diagnosis
- Give correct and appropriate management for each case
- Trigger the causes
- Correlate the reported symptoms
• Sixth nerve palsy is one of the causes of esotropia.
• In mild 6th nerve palsy, there is presence of limitation of abduction.
• The patient’s age is an important consideration, as an adult patient is unlikely to present with recent onset of distance esotropia, thus making 6th nerve palsy the likely diagnosis.
Example: left mild 6th nerve palsy
- In primary position : slight left esotropia due to unopposed action of left medial rectus
- Abduction : limit due to weakness of the left lateral rectus muscle.
- Adduction : Normal.
- Compensatory face turn : turn into the field of action of the paralyzed muscle (to the left) to minimize diplopia, so that the eyes do not need to look towards the field of action of paralyzed muscle (to the left).
- Associated with neurological disease.
Example : distance esotropia
- Near fixation : No deviation / small deviation
- Distance fixation : Small – moderate esotropia
(can be intermittent/constant esotropia)
- Abduction : Normal bilateral abduction
- Absence of neurological disease.
Q3: WHAT ARE DIFFERENCES BETWEEN FULLY ACCOMMODATIVE ESOTROPIA AND CONVERGENCE EXCESS ESOTROPIA
ReplyDeleteFully accommodative esotropia (refractive accommodative esotropia) likely to occur when accommodation is exerted to overcome uncorrected moderate hypermetropia.
The hyperope, in an attempt to accommodate or focus the eyes, converges the eyes as well. The over-convergence associated with the extra accommodation required to overcome a hyperopic refractive error can precipitate a loss of binocular control and lead to the development of esotropia.
In such cases, the esotropia will only be seen when the child removes their glasses. And BSV only present for near and distance if hypermetropia is fully corrected.
The main features:
1. Onset: 2-5yrs of age
Rare in aged 6month-2yrs/ >5yrs of age
2. Etiology: Degree uncorrected hypermetropia: 2-7DS BE
3. VA: reduce in deviating eye
4. Associated sign: rub/close eye
ET noticeable when child is tired/unwell
5. Intermittent ET will become constant ET if left untreated and resulting in strabismic amblyopia
Meanwhile in convergence excess accommodative esotropia with high AC/A ratio (nonrefractive accommodative esotropia) likely to occur on near fixation with refractive error corrected, due to excessive accommodative convergence exerted for each dioptre of accommodation.
Thus, in such cases, even when hyperopic refractive errors have been corrected, the child will continue to squint when looking at very small objects. Even though they are exerting a normal amount of accommodative or focusing effort, the amount of convergence associated with this effort is excessive, thus giving rise to esotropia.And BSV is present for distance fixation.
The main features:
1. Onset: 2-5yrs of age
2. Etiology: uncorrected hypermetropia (+1.5 to +5DS); emmetropia and myopia.
ET present in distance as well as for near until hypermetropia is corrected.
3. High AC/A ratio
4. Signs: ET noticed when child look up or when eating; child may close one eye
More noticeable when child is tired/unwell
5. VA: equal BE; any amblyopia present is likely to be associated with uncorrected
anisometropia
6. Microtropia associated with anisometropia
7. Suppression present when deviation manifest
8. Normal near point of accommodation
What are the differences between other intermittent esotropia and cyclic esotropia?
ReplyDeleteBoth of them seem same. But there are several differences between cyclic esotropia and other intermittent esotropia (accommodation & distance).
Cyclic ET is also known as circadian ET. Usually patient exhibit a large angle ET (50pd) followed by periods of normal sensory adaptation in a cyclic pattern. The pattern tends to be observed in a 48 hour rhythm which 24 hours of ET followed by 24 hours of normal binocularity. Aetiology is unknown and the onset is at 4 to 6 years old but after 6 to 12 months, the condition become a constant non accommodative esotropia, at which point the surgery usually performed. Cyclic esotropia maybe associated with condition of anxiety, depression, phobia or compulsive behaviour, which may also be cyclic. The method of assessment is slightly different compare to other types of intermittent ET. Patient has to come to the clinic during ET is manifest to measure the magnitude of ET and also come during not manifest to measure stereopsis.
For other types of intermittent esotropia, such as:
accomodation
• fully accommodative ET with normal AC/A ratio
• fully accommodative ET with CE (high AC/A ratio
distance
• near ET
• distance ET
they manifest at no specific condition. Usually a refractively corrected esotropia may breakdown these intermittent ET either by full or partial correction. In terms of onset, it depends on the types of intermittent esotropia. For example, fully accommodative ET with normal AC/A ratio, its onset is about 2 to 3 years and for fully accommodative ET with CE (high AC/A ratio), its onset is between 3 years old to 5 years old. The associated emotion problem is rare reported.
Why do you need to differentiate distance esotropia from mild 6th nerve palsy?
ReplyDeleteFrom my point of view,
We need to differentiate distance esotropia from mild 6th nerve palsy in order to
- Have a correct diagnosis
- Give correct and appropriate management for each case
- Trigger the causes
- Correlate the reported symptoms
• Sixth nerve palsy is one of the causes of esotropia.
• In mild 6th nerve palsy, there is presence of limitation of abduction.
• The patient’s age is an important consideration, as an adult patient is unlikely to present with recent onset of distance esotropia, thus making 6th nerve palsy the likely diagnosis.
Example: left mild 6th nerve palsy
- In primary position : slight left esotropia due to unopposed action of left medial rectus
- Abduction : limit due to weakness of the left lateral rectus muscle.
- Adduction : Normal.
- Compensatory face turn : turn into the field of action of the paralyzed muscle (to the left) to minimize diplopia, so that the eyes do not need to look towards the field of action of paralyzed muscle (to the left).
- Associated with neurological disease.
Example : distance esotropia
- Near fixation : No deviation / small deviation
- Distance fixation : Small – moderate esotropia
(can be intermittent/constant esotropia)
- Abduction : Normal bilateral abduction
- Absence of neurological disease.
CYCLIC ESOTROPIA
ReplyDelete-Cyclic esotropia is periodic convergence strabismus that often occurs every 48 hours.
It is also known as alternate day strabismus.
Q: HOW TO ASSESS PATIENT WITH CYCLIC ESOTROPIA?
Usually patients exhibit a large angle esotropia with sensory adaptation, followed by periods of normal binocularity in a cyclical pattern.
TEST
1)ONSET
-Mean age of onset is 3 to 4 years
-Eye rubbing or eye closure can be observed with the onset of this condition.
2)VISION ACUITY TEST
-Good and equal for both eye
3)OCULAR MOTILITY TEST:
-V pattern esotropia may be detected
4)REFRACTIVE ERROR
-Emmetropia to moderate hyperopia is present
5)COVER TEST (when no deviation present)
-Esophoria may be expressed during the periods of normal binocular vision.
6)COVER TEST (when deviation present)
-Large magnitude esotropia, equal at distance and near.
7)PRISM COVER TEST
-Approximately 50 PD (ref book: binocular vision by erik)
8)SENSORY ADAPTATION
-Supression and anomalous retinal correspondence may develop during episodes of esotropia.
-When aligned, patients generally exhibit normal retinal correspondence (NPC), good stereopsis and no strabismus.
9)AC/A RATIO
-High AC/A may be detected
QUESTION 2: WHY DO YOU NEED TO DIFFERENTIATE CONSTANT ACCOMMODATIVE ESOTROPIA AND INTERMITTENT ACCOMMODATIVE ESOTROPIA?
ReplyDeleteConstant accommodative esotropia : When the eye turn occurs at all distances and at all times
Intermittent accommodative esotropia : When the eye turn occurs only some of the time, the eye turn might be observed only occasionally, such as during stressful situations or when the person is ill. Up to the first 6 months of age, intermittent accommodative esotropia is a normal developmental milestone. After 6 months, it needs to be evaluated.
We need to differentiate between constant accommodative esotropia and intermittent accommodative esotropia because of the treatment that should be given to the patient.
Constant accommodative esotropia are to be dealt with immediately if one wants to re-establish proper use of both eyes (binocular vision). Treatment for this condition should be early and aggressive. If the eye turn is constant and simple things like patching, drops, and/or glasses (bifocal, prismatic, etc) do not eliminate the eye turn, Vision Therapy, Orthoptics, or Surgery needs to be considered.
With intermittent accommodative esotropia, the eye does not turn in all the time, so the brain is probably receiving adequate stimulation for the development of binocular vision. After 6 months of age, this condition does need attention, but neither the eye doctor nor parent needs to panic. As long as the eyes are straight some of the time, the brain will develop normal functioning of the eyes (stereoscopic depth perception). Children with intermittent eye turns should be handled with judicious patching, special glasses, and/or Vision Therapy. Surgery, if considered at all, should be a last resort.
Q4 : Why do you need to differentiate between fully accommodative esotropia and convergence excess esotropia?
ReplyDeleteFully Accommodative Esotropia (FAE) and Convergence Excess Esotropia (CEE) are both within the intermittent classification of esotropia.
FULLY ACCOMODATIVE ESOTROPIA
- It may onset by illness and from positive family history. Age between 2 to 5 years old.
- Those with moderate hyperopia, astigmatism and/or anisometropia.
- Cover Test show deviation without spectacle correction.
- Angle of deviation= a slight convergent angle is measure with glasses, increasing without correction and on accommodation.
- AC/A Ratio= normal.
- Management =give full correction after cycloplegic refraction. Treat amblyopia is present.
CONVERGENCE EXCESS ESOTROPIA
- Deviation inward when patient looking at close object. Age betweeb 2 to 5 years old.
- If due to uncorrected hyperopiaET at near and distance.
- Those with hyperopia and some myopia.
- Cover Test show deviation for near fixation on accommodation buy control maybe demonstrated.
- Angle of deviation= a slight convergent is measurable at distance fixation with a larger angle at near fixation.
- AC/A Ration= greater than 5:1
- Management= 1) Surgery required in high AC/A ration. 2) Orthoptic exercise for those co-operative children, AC/A ration less than 8:1, antisuppression exercise. 3) Bifocal. 4) Miotics that give larger depth of focus to less accommodation required. 5) Contact lense useful with high AC/A ratio and those associated with myopia.
HOW TO DIFFERENTIATE BETWEEN THE CONVERGENCE EXCESS ESOTROPIA AND NEAR ESOTROPIA?
ReplyDeleteThere are different aspects for these two types of esotropia, so it needs to be differentiated.
Convergence Excess Esotropia
DESCRIPTION :
*Normal BSV at distance,
esotropia on ACCOMMODATION FOR NEAR FIXATION.
*a.k.a accommodative convergence excess
AETIOLOGY:
*High AC/A ratio
*Remote neAr point of accommodation
Near Esotropia
DESCRIPTION :
*Normal BSV at distance,
esotropia at near IRRESPECTIVE ACCOMMODATION.
*a.k.a non-accommodative convergence excess
AETIOLOGY:
Excess tonic vergence
Thus, I think to differentiate between the convergence excess esotropia and near esotropia, it is essential TO DETERMINE THE ROLE OF ACCOMMODATION in causing the increased near deviation & in term of AC/A RATIO.
1st: :)
-->Add +3.00DS to patient’s prescription
-->Perform cover test at near : to measure the deviation with addition +3.00DS
Finding:
**CE Esotropia: Esodeviation reduced/eliminated
**Near esotropia:Esodeviation maintain
the same
2nd: :)
-->Perform cover test using accommodative target
--> the deviation is measured while the patient fixates on an accommodative target at 33 cm distance.
Finding:
Finding:
**CE Esotropia: Esodeviation reduced/eliminated
**Near esotropia:Esodeviation maintain
the same
3rd: :)
--> Add +3.00DS to patient’s prescription
--> Perform cover test at near : to measure the deviation with addition +3.00DS while patient fixate on accommodative target at 33cm
--> AC/A ratio is measured using the gradient method
Finding:
CE Esotropia:
Esodeviation reduced -> high AC/A ratio
Near esotropia :
Esodeviation maintain the same->low AC/A ratio
~~for the 3rd method, i think the Modified Thorington technique also can be applied, refer to Essential Clinical Binocular Vision, Erik M.Weeissberg, pg 153~~
comments are welcome~~(^__^) v
Question : How do you diefferentiate between infantile esotropia and pseudo-esotropia?
ReplyDeleteInfantile esotropia is usually be confused with pseudo-esotropia. The two syndromes mostly affect the infants and toddlers. However, the are several ways to differentiate between infantile esotropia and pseudo-esotropia. It is included theorical and practical part. We can differentiate the two cases by definition, causes and possible treatment that can be implemented to the patients. While, in the practical part, the differences can be found from the signs and clinical test that can be suggested to diagnose the syndrome.
Practically, we can differentiate between infantile esotropia and pseudo-esotropia through certain clinical tests. It include hirscberg test, cover and uncover test. Usually when we do these tests, pseudo-esotropia will show no deviation in the eye. The corneal light reflex test, such as shining a flashlight in the patient's eyes from 3 meters away and examining the light reflex on the cornea, can be performed to differentiate pseudoesotropia and true esotropia.
1)Infantile Esotropia 2)seudo-esotropia
DEFINITION
1)is a condition in which the alignment of the eyes is straight (also known as orthotropic. however, they appear to be crossed.
2)is the inward deviation of the eyes noted before the patient reaches age 6 months
CAUSES
1)Unknown. However, The exact cause of infantile esotropia has yet to be identified distinctively. While it strongly is believed that a genetic component exists, a solid basis for linkages among family members still needs to be established. Furthermore, large-scale investigations have shown that 20-30% of children born to a strabismic parent eventually will develop strabismus themselves.
2)This condition most commonly occurs in infants when a flat nasal bridge and prominent epicanthal folds tend to obscure the nasal portion of the sclera. This optical illusion causes the patient to have an appearance of eyes deviated nasally, and it is most apparent when the eyes are in side gaze or are focusing up close. A small interpupillary distance (for example the distance between 2 pupils) also can give the appearance of pseudoesotropia.
@The Traveler
ReplyDeleteOK.
hafizah, since I did the same topic with u..i would like to add..
ReplyDeletethis CE ET and Near ET need to differentiated carefullly, since it actually involve diiferent aetiology, deviation accurred differenly : accommodation factor..so there will be no mis-interpratation b/n this two 2 types ET, as u explained here which the efficeint treatment & management can be given..
hehe...detailed can be read on bro muzy note, references book...(^__^)
sorry sir, i totally forgot to post this assignment before.
ReplyDeleteQ9 : How do you differentiate distance esotropia from mild 6th nerve palsy?
Distance esotropia is a form of strabismus which cause the eyes to turn inward and give the cross eyes appearence while 6th nerve palsy is a disorder associated with dysfunction of the abducens nerve which is responsible for contracting the lateral rectus muscle to abduct or turn out the eye.The affected individual will have an esotropia or convergent squint on distance fixation.
Esotropia patient will only have reduction in vision in one or both eyes or sometimes diplopia and the brain will suppress the image from the esotropic eye in order to relieve the symptom, but as for the 6th nerve palsy patient, they sometimes adopt a face turn towards the side of the affected eye, moving the eye away from the field of action of the affected lateral rectus muscle, with the aim of controlling diplopia and maintaining binocular vision.
Your Blog is Really Nice. you have sharing the Really Good Information.
ReplyDeleteDr Madhu Karna Eye Specialist in India.